Table of contents
Personal Note
Compound description and mechanism of action
MK-677 Desired Effects and Uses
Effect on Muscle Mass
Effect on Sleep
Effect on Injury treatment and prevention
Effect on BMR
Effect on Hair
Effect on Immune Health
Effect on Bone Health
Effect on Cognition
Effect on Hormones
Effect on Skin and Facial Aging
Mk-677 Side Effects
Effect on Blood Glucose/Insulin Sensitivity
Effect on Appetite
Effect on Addiction
Effect on Water Retention
Effect on Joint pain
Effect on Acne
Effect on Blood Pressure
Effect on Cancer Cells
Effect on Gynecomastia
Effect on Lethargy and Brain Fog
Effect on Epigenetics
Miscellaneous
Personal Note
I have never used MK-677 and I’m not affiliated with any SARM manufacturers/suppliers, and do not encourage its use. All information used is based on research, of which is cited. If information is missing a citation email intelligentpersonaltraining0@gmail.com and the citation will be provided to further your own personal research.
Compound description and mechanism of action
Mk-677 or Ibutamoren is an orally active growth hormone secretagogue (GHS) and ghrelin receptor agonist. GHS’ are a class of drugs that are named after GH because the hormone Ghrelin wasn’t yet discovered, but they basically mimic the hormone Ghrelin in order to secrete GH.
A growth hormone secretagogue is any compound that signals to the pituitary gland of the brain to release growth hormone (GH). So it is not a source of exogenous hormones taken orally, but rather a compound that signals to your body’s natural mechanisms to increase the amount of GH secretion.
How does MK-677 stimulate GH release? By mimicking the action of the hormone ghrelin and binding to GHSR-1A (a growth hormone secretagogue receptor) in the brain, which stimulates the release of GH.
One of the actions of GH is the secretion of IGF-1 (insulin-like growth factors) in the liver. There are two IGF’s, but IGF-1’s corresponding receptor (called literally the ‘IGF-1 receptor’) is the “physiological” receptor and GH/IGF-1 has be taken experimentally in body building circles for the physiological changes it promotes such as muscular hypertrophy, by inducing protein synthesis, and additionally by blocking muscle atrophy (the breakdown of muscle tissue).
- This interplay between growth hormone (GH) and insulin-like growth factor 1 (IGF-1) is called the “IGF-1/GH axis”.
However it has lots of other effects within the body, positive in negative, which will be explored in detail.
Other notable details about the compound is MK-677 has a half life of 6 hours, but the IGF-1 levels remain elevated in humans with a single oral dose for up to 24 hours, allowing for a convenient daily administration. MK-677’s administration timing is also something that will be examined later. Unlike synthetic growth hormone administration, MK-677 does not suppress the body’s natural production of growth hormone.MK-677 research has been centered around its potential to treat conditions associated with growth hormone deficiency such as muscle wasting, osteoporosis, and age-related frailty due to its anabolic and regenerative properties. However, note that MK-0677 is not currently approved for clinical use by any regulatory agencies.MK-677 is also known by the following names; Ibutamoren, MK-0677, L-163191, LUM-201.
MK-677 Desired Effects and Uses
EFFECT ON MUSCLE MASS
The most recent study on MK-677, from 2022, studied the effects of coadministration of it and LGD-4033 (a SARM) on a 25 year old male with previous weightlifting experience for 5 weeks. This coadministration was shown to have the following effect on muscle mass:
- Increase in total lean body mass (mass of everything except fat), +3.1%;
- Increase in trunk lean body mass (lean mass in trunk area -chest/back/abdomen-), +6.6%;
- Increase in appendicular lean body mass (lean mass in arms and leads), +4.3%

Although these results are substantial for 5 weeks, for a male with previous years of weightlifting experience, most of this would probably be attributed to LGD-4033 as it is a SARM. A key drawback of this study is its sample size, as it was literally a study on 1 patient however it does add to the body of research about MK-677s effect on body composition, and interesting to look at anyways.

A 2008 2-year, double-blind, randomized, placebo-controlled clinical trial on 65 older adults on MK showed the following results.
The MK-677 group experienced a significant increase in fat-free mass (+1.1 kg) compared to the placebo group, which saw a decrease (-0.5 kg) over 24 months.
- Mk was taken at 25mg per day
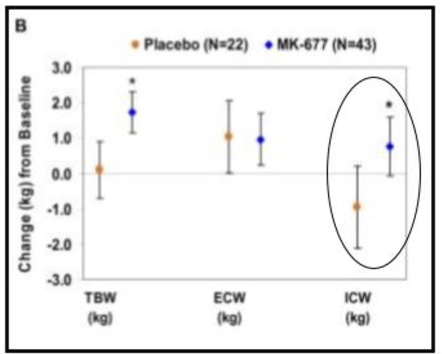
However this wasn’t pure contractile muscle tissue as there was also an increase in intracellular water (+0.8 kg in the MK-677 group vs. -1.0 kg in the placebo group).
Also, the muscle gained in the first year by ‘Group 2’, declined after placebo administration, so increased gains made while taking MK are likely to be temporary.
A 1998 double-blind, randomized, placebo-controlled clinical trial focused on its ability to prevent diet-induced catabolism.
During the period when participants were both calorically restricted and taking 25mg MK-677 (after 7 days), their nitrogen balance improved significantly (+0.31 g/day) compared to those taking a placebo, who remained in a negative nitrogen balance (-1.48 g/day). This suggests that MK-677 helped prevent muscle breakdown and supported muscle maintenance or growth under calorie-restricted conditions.

- Nitrogen balance is a key indicator of muscle growth or loss, as it reflects the balance between protein intake and protein breakdown in the body.
As seen from the figure, there was an increase in Nitrogen balance after MK-677 was administered on the 7th day.
Another 1998 double-blind, randomized, placebo-controlled clinical trial focused on its effects on 24 obese men. The study found that after eight weeks of treatment, subjects who received MK-677 experienced an increase in FFM of approximately 3 kg compared to the placebo group. This study considered water weight and mentioned that “the increase in FFM is not explained by an increase in body water”, however they also acknowledge shortcomings in methodology, saying that difference in measures of water weight may explain about half of the increase in FFM.

- A more accurate conclusion from this study would of been ~ 1.5kg increase of FFM, which is a moderate-good result for 8 weeks of a compound for muscular hypertrophy
Anecdotally, many users attribute most of their lean weight gain to water retention, and report huge increases in weight the first week of usage.
There aren’t many human studies that directly look at how MK-677’s effects build muscle, but there is a wide body of research that supports how IGF-1 leads to muscular hypertrophy and improved body composition, so by extrapolation we can see the effects MK-677 may have.
The signaling pathways by which IGF-1 promotes hypertrophy is as follows.
Once IGF-1 binds to the IGF-1 receptor (IGF-1R) the receptor mediates the phosphorylation (a process typically well known as enzyme activation), of a intracellular adaptor protein IRS-1 (insulin receptor substrate-1) which then recruits and phosphorylates phosphoinositide 3-kinase (PI3K) followed by Akt phosphorylation.
According to a few studies, like this study from 2001, this PI3K/Akt pathway plays a critical role in myotube hypertrophy.

IGF-1 signaling inhibits the activity of GSK3β, an enzyme that normally suppresses protein synthesis. Inhibiting GSK3β leads to the activation of eIF2B and β-catenin, both of which are involved in muscle hypertrophy.
IGF-1 also interacts with other signaling molecules in the regulation of muscular hypertrophy, notably myostatin. Myostatins suppressive effects on building muscle have been well studied, and it is known that it acts to prevent excessive muscular growth – essentially as a barrier.
An extremely interesting phenomenon which initially led to this line of research is the ‘Belgian Blue Cattle’, which had extremely abnormal muscle mass compared to other cattle. It was found that this phenomenon was due to a natural mutation in the myostatin gene (a suppression of myostatin), which increases muscle fiber number, leading to a leaner, more muscular build.
Another notable thing about this case is that myostatin deficiency leads to an increased number of muscle fibers (hyperplasia), instead of the (normal) enlargement of individual muscle fibers (hypertrophy).
According to a few studies IGF-1 counteracted the suppressive effects of myostatin on hypertrophy, and IGF-1’s general hypertrophic effect was enhanced when Myostatin was inhibited.

This is a very obscure topic and amongst bodybuilding circles this doesn’t seem to be discussed at all, but through extrapolation the hypertrophic effects caused by IGF-1 through Gh administration or GHS like MK-677 may be improved when a myostatin inhibitor like YK-11 is introduced. However it is important to note that this is just speculative and both compounds are not approved for human usage at this current date.

When muscle building is discussed, the main method on which this occurs is ‘hypertrophy’ – the enlargement of individual muscle fibers, but there is another process called ‘hyperplasia’ – an increase in the number of individual muscle fibers. Currently IGF-1 is the only known hormone to create new muscle fibers.

My concluding thoughts on MK-677’s effects on muscle growth is that it has mild-moderate muscle building potential but not a needle mover. However IGF-1’s (and thus MK-677’s) ability to promote hyperplasia is interesting and may serve to create a synergistic effect with anabolic agents which can cause hypertrophy, as well as its enhancing effects when myostatin is inhibited. It could be useful to prevent muscle catabolism in a calorie deficit but this is very debatable because some of its side effects make it very hard to remain in a deficit (see sections on effects on lethargy and appetite), but if you have the willpower it may be useful for this use amongst those who don’t want to take AAS.
EFFECT ON SLEEP
The relationship between growth hormone (GH) and sleep operates as a positive feedback loop, where each one enhances the other. This feedback loop ensures that adequate rest enhances GH production, which supports recovery, tissue repair, and overall health, while elevated GH levels contribute to better sleep quality, forming a cycle of mutual reinforcement.
MK has an extremely positive effect on sleep duration and quality, shown in a few studies which will be examined. In my opinion this is the most underappreciated effect of MK. The positive relationship between sleep and strength/hypertrophy has been well established. Hence MK-677 might indirectly improve muscular hypertrophy and strength, especially in those who struggle to get 7+ hours a night.

GH secretion naturally peaks shortly after sleep onset, particularly during the first period of SWS (slow-wave sleep), which is the deepest phase of non-REM sleep. MK-677, by enhancing GH secretion, may promote more frequent or intense episodes of SWS (a part of sleep important for muscle recovery).
From what I’ve seen, most recreational users find that while using MK-677 they find it easier to fall asleep and experience much deeper sleep. It is also pretty common for some users to experience a feeling of refreshment when they wake up, but this isn’t as frequently mentioned. Some guys will also start having lucid dreams shortly after starting MK.

This phenomenon is also present in scientific literature. A 1997 study on MK found that when dosed at 25mg there was a 20% increase in REM sleep amongst young men, and a 50% increase in REM sleep amongst older men, both of which were statistically significant changes when compared to the placebo group.
INJURY TREATMENT AND PREVENTION
Injury treatment:
GH and IGF-1 have been shown in studies to be beneficial for injury treatment in tendons and ligaments, like this one from 2023. Obviously this effect would extend to MK-677.

Also the sleep benefits that MK-677 provides are almost sure to help aid injury recovery. I’m not going to go into this point because I’m sure everyone is aware of sleep’s regenerative effects.
Injury prevention:
In a study from way back in 1967 researchers were interested in GH’s effect in treating bodily trauma, specifically on burn victims. It was found that potassium balances generally became more positive during HGH administration, indicating a potential for preferential increase in intracellular water (ICW).

- A high ICW content has been loosely shown to improve frailty and act to treat/prevent injuries
- Its thought to do this by maintaining synovial fluid which lubricates joints
- Anecdotally it’s quite common for bodybuilders to get injured during the last week of dieting for a show when they are being water depleted
The administration of MK-677 to secrete GH may be a way of extra injury prevention, although I think there are better compounds for this, and as mentioned before it is extremely counter-intuitive to use MK-677 during a dieting phase.

Anecdotally many powerlifting report GH to not be protective measure for injuries and in fact many report joint pain, however this may be a by product of its healing effect on existing injuries
My concluding thoughts about MK-677 in the context of injury treatment and prevention, is that it provides some effect on injury treatment, however there are far more effective compounds notably BPC-157. It is more promising in the context of injury prevention, and would probably be better utilized in a ‘bulk phase’ as an extra safety net. Anyone that has experience with this compound can confirm MK is very difficult to use in a ‘cutting/dieting phase’.
One of the biggest things overlooked about MK-677 is its synergistic effect when combined with BPC-157 for injury treatment. When studying BPC-157, researchers noticed a 2.29x increase in gene upregulation of the growth hormone receptor in tendon fibroblasts.

This effect is observed at both the mRNA and protein levels and increases in both a dose and time dependent manner. This increase in growth hormone receptors can work synergistically with increased growth hormone. Additionally after growth hormone binds to the growth hormone receptor it activates the Jak2 (Janus Kinase 2) signaling pathway, which plays a key role in mediating the growth-inducing effects of GH. Interestingly, in BPC-157 treated tendon fibroblasts, the growth hormone led to more significant activation of the Jak2 signaling pathway, demonstrating a 1+1=3 synergistic effect of GH and BPC.

EFFECT ON BMR
For those unaware BMR stands for Base Metabolic Rate, and it basically measures how much energy your body expends when you are doing nothing (i.e. lying around on the couch watching a show with nothing being digested.
This is why whenever somebody who is skinny or has a low body fat percentage talks about how they eat so much the typical response you’d hear is that they must have a ‘fast metabolism’.
There are a few studies on GH’s effects on increasing BMR, with this one from 1994 in prepubertal boys showing that it when adjusting for weight fluctuations it increased significantly after two months of treatment, then stabilized;
- REE stands for resting energy expenditure, which is essentially BMR

These results can also be seen in two studies from 1991 and 2019 on prepubertal boys. With the one from 2019 also showing that this increase of BMR occurs after 6 weeks.


Unsurprisingly MK itself has similar effects on BMR as GH, with a 1998 study exploring this relationship (on obese patients). This study found that MK administration did in fact significantly increase BMR, but one of the key difference in its effects, compared to traditional GH administration, is that the increase in BMR was seen faster (after 2 weeks for MK, rather than 2 months for GH administration).

This graph shows the difference in BMR – corrected for body mass – after 8 weeks, between MK-677 administered and placebo group.

It is important to note that these results were found on obese men, and it may not yield the same results based on your individual body composition, however if we were to extrapolate these results for non-obese men MK-677 would affect BMR in the following ways
- If you were a 100kg male, after two weeks your BMR would increase by ~ 150 kcal
- However this increase would stabilize thereafter
- MK-677 worked faster to increase BMR than traditional GH administration
I find it quite intriguing how researchers looked at MK-677s effectiveness as an obesity treatment, despite it being a Ghrelin Agonist and having an obvious effect on appetite. It goes to show that there is a place to consider anecdotes because all these early studies on MK didn’t really report its effects on appetite which in practical application is an extremely counterintuitive obesity treatment.
EFFECTS ON HAIR – HAIR LOSS TREATMENT?
An 2021 article called “Growth Hormone and the Human Hair Follicle” explored this relationship in great depth.

They conclude that excess GH clinically causes greater hair growth in men, whereas in females certain effects of GH may outweigh this benefit. The mechanism by which it promotes greater hair growth in men is through IGF-1 which generally promotes a more potent anagen (growth phase) prolonging factor in hair follicles. An increase of the anagen phase in hair follicles can help your hair look thicker.
Another study in 2018 looked at how GH influences HF biology through its interactions with the hypothalamic-pituitary-somatotropic (HPS) axis. It similarly concluded that humans with GH deficiency have diminished results to hair loss treatments like Finasteride and Minoxidil, due to a lack of IGF-1, and suggest that it may play a complex role in HF growth cycles.
Anecdotally, a lot of users report greater hair growth, and better hair density when on MK-677. While this is a positive, GH and IGF play no part in treating the root cause of androgenetic alopecia which is caused by DHT binding to scalp hair follicles and transcribing its effects leading to hair follicle miniaturization. Cosmetically MK-677 will make your hair look better and thicker not because it treats hair loss, but because unaffected hair follicles will have prolonged growth phases. This may be an important factor for those looking for a substance that ‘boosts’ performance enhancement without detrimental effects to hair follicles, which are commonplace for people running certain cycles and protocols of anabolic steroids, but for most this is just a fringe benefit they notice whilst on it. What is clear from the studies is GH treatment will have the greatest effect for those who are already GH deficient, but I’d speculate that the effects would be mild if you have a normal amount of GH and IGF-1.
If you are interested in treating hair loss check out articles here.
EFFECTS ON IMMUNE HEALTH
There hasn’t been a complete picture painted about its effects on the immune system, however there are a few takeaways we can make from studies.
A study published in 2023, looked into treatment using L-163,255 ‘a close analog to MK-677’ and noticed an increase in thymic cellularity and differentiation in older mice.

This essentially means that when treated with GHS the thymus (an organ important for the immune system) has more cells, and those cells are developing into specialized immune cells more effectively in older mice.
The study also found that GHS treatment enhanced antibody responses (antibodies serve to eliminate pathogens) in old mice and made them more resistant to tumor initiation (a process in which normal cells are changed so that they are able to form tumors) and metastases (the spread of cancer to a new part of the body).
Additionally the study found that a GHS treatment helped more of these bone marrow cells settle in the thymus in mice, which means that the thymus can produce more T-cells. This is a positive effect on the immune system because T-cells are crucial for fighting infections and diseases, and having more of them helps improve overall immune response
Finally, the study found that GHS can play a role in the Regulation of pro-inflammatory cytokine expression.
Ghrelin and its receptor, GHSR1a, are expressed in T cells.
The study indicates that ghrelin acts in both autocrine and paracrine ways to regulate how pro-inflammatory cytokines are expressed in mouse and human T cells.
For those without an understanding on T cells and immunity biology here is a brief extract taken from this website, explaining how these processes work in simpler terms.

EFFECTS ON BONE HEALTH
A study from 1998, studied the effects of MK-677 on bone health over a period of two months. Although they noticed improvements in markers used to measure bone health they acknowledged the limiting factor being the study duration.
This is because in other studies, it took 18 months for an increase to be seen in BMD (bone mineral density) for patients treated with GH.

This was replicated in a study from 1999, which suggested MK-677 had positive effects on bone health, but once again was a short term study, and longer term studies are needed to know for sure.
COGNITIVE EFFECTS

There has been a link established between GH and cognitive function. Researchers speculate that there is a correlation between the age-related decline in cognition and age-related decline in GH.
According to an article from 2023, there are some mechanisms by which GH improves cognitive function.
GH can activate neural stem cells (NSCs) in the adult brain. This can lead to an increase in the number of neurons in key regions of the brain, particularly the hippocampus, which is critical for learning and memory
GH can induce BDNF expression. BDNF (brain-derived neurotrophic factor) is a protein that plays a role in learning and memory functions.

It can also be neuroprotective. Many of the other studies reviewed in this article are on GH deficient adults, so there is potential GH’s positive effects on cognition are related to treating an underlying deficiency but having elevated levels may not have a dose-dependent effect on cognitive performance. Speculatively, there probably is little to no effect on cognitive enhancement amongst young males who have much higher GH levels than older men, aside from the fact elevated levels may be neuroprotective.
One topic commonly discussed about MK-677 in bodybuilding communities is its potential to cause brain damage and PTSD. This was incorrectly extrapolated from a 2014 study on rats titled ‘A ghrelin-growth hormone axis drives stress-induced vulnerability to enhanced fear’. There are a few problems with the study, and problems with how its been extrapolated to infer potential effects on human biology. In the study they both inject, and infuse MK-677 into the brains of the rats, which is extremely different to the oral administration seen in humans. Although the study did show it did increase markers in fear memory, we have extremely different biologies to rats so this is extremely poor evidence to make this claim. We also have year long studies on MK-677 with no reports of a fear or anxiety inducing effect, and it hasnt really been reported anecdotally either.
EFFECTS ON OTHER HORMONES
A common reason why in bodybuilding circles, MK-677 is seen as a gateway to other compounds, or is usually the compound guys use to ‘dip their toes in the water’, is because it does not suppress endocrine function so there isn’t a ‘crash’ in endogenous hormones seen in anabolic steroids.

According to a 1999 study, MK-677 did not affect free testosterone levels or FSH and LH (which regulate the production of testosterone).
The reason for this is MK-677 does not affect the hypothalamic-pituitary-gonadal (HPG) axis.
Growth hormone and male sex hormones (i.e testosterone) are regulated by different mechanisms in the body. Testosterone production is controlled by the hypothalamic-pituitary-gonadal (HPG) axis. The hypothalamus releases GnRH, which signals the pituitary gland to release LH and FSH, which activate the testes to produce testosterone. MK-677 does not interact with this pathway. It acts solely on the hypothalamic-pituitary-somatotropic (HPS) axis, which is involved in regulating growth hormone production.

A very interesting article published in 2020, suggested that ibutamoren and other GHS may be helpful in treating specific hypogonadal symptoms (a condition that affects the ability of men’s bodies to produce enough testosterone), despite them not interacting with the HPG axis.
It should be noted that Ghrelin has been shown to inhibit the secretion of gonadotropin-releasing hormone (GnRH) which is involved in Testosterone production, however this negative result has not been reproduced in any human trials on MK-677.
EFFECT ON SKIN AND FACIAL AGING

As you know, MK-677 increases IGF-1 in your body. Thus the benefits of increasing your IGF-1 would likely apply for MK-677 administration, even if there aren’t any studies that investigate these specific effects with MK-677 administration. One of IGF-1s effects is the improvement of skin health.
A study measuring how IGF-1 bioavailability correlated with decreased perceived skin aged, showed its positive effects on skin aesthetics.
The difference was small but still statistically significant.
However, as discussed later in the side effects section, IGF-1 (MK-677) may cause acne thus decreasing skin aesthetic, so ultimately it is up to users discretion.
MK-677 Side Effects
Before getting into the side effects, there are some common limitations with MK-667 usage.
There are many drugs that can’t be used by specific people due to genetic and physiological differences, and that is quite common. For example, Finasteride typically isn’t prescribed to children because DHT plays a significant role in puberty and sexual development.
But with MK-677 there is a very wide range of people who can’t, or shouldn’t use it. These include:
- Individuals who don’t have a functioning hypothalamic pituitary adrenal (HPA) axis.
- Individuals with high blood sugar / type 2 diabetics (or those with a genetic predisposition to type 2 diabetes)
- Individuals with high blood pressure
- Individuals who are unable to secrete growth hormone
EFFECTS ON BLOOD GLUCOSE/SUGAR AND INSULIN SENSITIVITY
In a 2008, two-year randomized controlled trial involving healthy older adults (60-81 years old), daily administration of MK-677 (25 mg) led to a statistically significant increase in fasting blood glucose levels. On average, fasting blood glucose increased by 0.3 mmol/L (5 mg/dL) after 12 months of MK-677 treatment compared to the placebo group.

- The increase was sustained over the two-year study period, although it was not statistically significant when compared to baseline values at the end of year 2

As mentioned, the average increase in fasting blood glucose was relatively mild. However a smaller subset of patients experienced more noticeable increases.
The study also noted that in patients insulin sensitivity decreased.
One of GH’s effects is to increase blood sugar levels by reducing the uptake of glucose into muscle and fat cells and promoting gluconeogenesis in the liver, which is the production of glucose from non-carbohydrate sources.
When growth hormone levels are consistently elevated, it forces the pancreas to work harder to produce and release sufficient insulin to counteract the rise in blood sugar. Insulin is produced by the beta cells of the pancreas. The continued demand for insulin due to the chronic elevation of growth hormone can lead to what is known as “pancreatic stress”, and the beta cells can become overused and degenerate. This is how type 2 diabetes is developed.
The abuse (or even introduction in certain individuals) of MK-677 or synthetic growth hormone can amplify this effect, potentially pushing the individual into a diabetic state sooner than they would have otherwise experienced, or just generally increase their likelihood of becoming diabetic. As you can imagine, this is not a compound you should consider taking if you have type 2 diabetes or a genetic predisposition to this condition.
There is a case report of this phenomenon

EFFECTS ON APPETITE

The most commonly reported side effect of MK-677 in studies was an increase in appetite.
It is pretty common for anecdotes to report that taking 25mg of MK-677 daily meant that it was basically impossible to eat enough food to feel satisfied.
Remember, MK-677 works by mimicking the action of the hormone ghrelin and binding to GHSR-1A (a growth hormone secretagogue receptor) in the brain, which stimulates the release of GH.
Ghrelin within the body is referred to as the hunger hormone, and although it is one of the misunderstood hormones and performs a variety of other functions, it is true its main function is to regulate hunger.
Ghrelin activates specific cells in the anterior pituitary gland and hypothalamic arcuate nucleus, with neuropeptide Y neurons being the one that initiates appetite.
As you’d expect, taking a compound that mimics ghrelin will cause you to feel hungrier than you normally would, and it’s been shown in investigative science that obese people tend to have higher natural levels of ghrelin.
Because of its effect, it’s commonplace for individuals in bodybuilding circles to take MK-677 to increase appetite in order to increase their daily caloric intake so they can pack on more muscle.
However what is overlooked is other types of Growth Hormone Secretagogue have lower elimination half life, such as GHRP-6 of 2.5 hours, and can be employed before eating a specific meal you wouldn’t be able to and have this increases appetite effect for a shorter period in order to eat more, and not have to experience the effects of having a greater appetite for the entire day. This is speculative, and is definitely not a recommendation because at the end of the day MK-677 has the most human data out of all the GHS.
Another GHS worth mentioning is Adenosine, which is able to increase appetite, unlike other agonists of this receptor, but is unable to induce the secretion of growth hormone and increase its plasma levels. Interesting Caffeine (Methylxanthines) has a structure which binds to the same receptors as Adenosine, and has been shown to be a competitive antagonist of adenosine and can blunt its pharmacological effects, so maybe this explains why some people feel an appetite suppressant effect from coffee.
Many from bodybuilding circles don’t consider how potent this effect is, making it almost impossible to stay in a calorie deficit. This is likely why companies stopped pursuing it for its treatment of obesity and now it is being looked at for treating PGHD (a rare condition causing growth hormone deficiency in children).

Many of the studies noted an increase in body fat.
MUSCLE PAIN

EFFECT ON ADDICTION – POTENTIAL ADDICTION TREATMENT?
A side effect I have never even seen discussed is the possibility for MK-677 to cause or treat addiction. Ghrelin has been shown to activate the cholinergic-dopaminergic reward link and ghrelin receptors are found in neurons in the reward system, including the ventral tegmental area (VTA).
- In mice that received ghrelin injections to the third ventricle, the VTA, or the laterodorsal tegmental area (LTDg), there was an increase of extracellular dopamine in the NAcc (nucleus accumbens – a area of the hypothalamus that plays a significant role in the cognitive processes of motivation, aversion and reward)
The mesolimbic reward system is significantly affected by short and long term exposure to addictive substances. Ghrelin plays a role in modulating behaviors involved in the in acquired natural rewards like food through its hunger signaling role, and it’s been proposed by researchers and experts that it amplifies behaviors that lead to the acquiring of artificial rewards, for instance DRUG SEEKING, by acting essentially as a craving trigger.
This is somewhat out of my depth, but it seems to be that the evidence is conflicting when it comes to how treatments that involve GHS-R1A agonists interact with addiction.
As you can see below (abstract from ‘The role of ghrelin in addiction: a review’) there are quite a few rodent studies that show GHS-R1A agonists may in fact treat addiction, specifically to alcohol.

What this suggests is that although GHS-R1A agonists like MK-677 mimic Ghrelin, they do not cause the same effect as Ghrelin in the brain in regards to the modulation of addiction.
There are no studies that I’m aware of that look directly at MK-677 and addiction, but there have been inquiries made using other GHS-R1A agonists, namely JMV2959. This 2021 study demonstrated that JMV2959 may be an effective treatment to treat drug addiction.

It’s an interesting concept and there needs to be further research to make accurate assessments of how MK-677 and other GHS-R1A agonists affect you cognitively.
EFFECT ON WATER RETENTION
There is a long studied connection between HGH/IGF-1 and an increase in water retention. The first I’m aware of is from the 1967 study on burns victims I mentioned previously. It was observed that potassium levels became more elevated during HGH administration, indicating a potential preferential increase in intracellular water.

In a 1999 study titled growth hormone and fluid retention, researchers concluded that GH administration was an effective treatment of chronic dehydration – a prevalent side effect of GH-deficient subjects. However the increase in water retention from GH doesn’t taper at higher levels. So when someone with normal GH levels at their age takes MK-677 they will experience increased water retention on top of the regular levels they had pre-treatment.

In anecdotal logs amongst bodybuilding circles, probably the most common side effect is extreme water retention. This is reflected through the following symptoms;
- Puffy face
- Extreme pumps in the gym – this sounds good but it is just the manifestation of the water retention side effect
- Swelling around the abdominal region
- Swelling around ankles
Some note extreme joint pain around the knees and ankles, making it very hard to walk. This symptom can be considered a separate side effect but it is basically a result of increased water retention. Most note that the extreme increase in water retention subsides after about a week.

In the 2008 study on 65 patients taking MK-677, the most common reported side effect aside from an increase in appetite was mild lower extremity edema and muscle pain.
It is highly likely that by taking MK-677 you will experience some degree of swelling or symptom of water retention, andit’s likely that this swelling could to lead to serious health consequences itf used for prolonged periods recreatioanlly
EFFECT ON JOINT PAIN
Acromegaly, is a condition where the body produces too much growth hormone after childhood (when there is too much growth hormone produced during childhood this leads to a different condition known as gigantism). In most cases this is caused by a tumor in the pituitary gland.
As mentioned before, a common symptom reported anecdotally from MK-677 is joint pain, particularly in the knee and ankle region. This is consistent with one of the symptoms of acromegaly being constant joint pain. When you think about it, by taking MK-677 (particularly in the first few weeks) you are inducing a temporary state of Acromegaly – assuming you already have regular levels of GH/IGF-1 prior to taking MK.
So your going to experience a lot of the mild symptoms of Acromegaly, and speculatively if you take MK-677 for a prolonged period of time, like 5+ years for example you’re going to start to develop the more serious symptoms associated with acromegaly that take longer to actualise.
I can’t find any mention of joint pain within the human trials on MK-677 but there is a very simple explanation for why some individuals report this.
When the body retains excess water, there may be an increase in swelling in soft tissue around the joints. This swelling increases pressure on the joints, particularly in weight-bearing areas like the knees, ankles, which unsurprisingly is where most report their joint pain.
Additionally, it is no secret that most people have a huge total body weight increase initially after taking MK-677, just by having a sudden increase in body weight from fluid retention, your joints simply put have more load to move around and they do not grow as fast proportionally to tissue especially when using PEDS.
EFFECT ON ACNE
This is another potential side effect I haven’t really seen discussed, including with people who did deep dives into MK-677 and other PEDS. There are a few studies that link IGF-1 to Acne. This article from 2017 explores the strong correlation between the western diet (of which increases insulin and IGF-1) and the development of Acne. It explores the proposed mechanism by which this occurs; essentially IGF-1 upregulates inflammatory biomarkers in sebaceous glands. For people also interested in skin health this is an extremely interesting article.

EFFECT ON BLOOD PRESSURE
A common side effect of edema is an increase in blood pressure. I’m going to explore how this could occur on MK-677, but also explain why I don’t believe this is likely for someone taking MK-677.

There are two reasons for why blood pressure may increase from MK-677, and both may be true at the same time.
- It is likely the volume of fluid in the bloodstream increases, which would lead to a higher blood volume. Blood pressure is partly determined by the amount of blood circulating in the vessels, so by having more blood means the heart has to work harder to pump it.
- Fluid retention is often tied to the activation of the RAAS system, which is a hormonal pathway that helps regulate blood pressure and fluid levels. When the kidneys sense a drop in blood flow or pressure, they release renin. This kicks off a chain reaction that produces angiotensin II and aldosterone. Angiotensin II causes the blood vessels to tighten, while aldosterone makes the kidneys hold onto more sodium and water. This ultimately leads to more blood volume and higher pressure in the blood vessels.
However, in this study from 2002, on 10 adults, researchers concluded the increase in ECW after GH strangely didn’t change or even in some cases decreased blood pressure.

Additionally, a 2020 study on 1094 subjects, reviewed the association between GH/IGF-1 and hypertension – with one of the metrics used to measure this being diastolic blood pressure.

The paper found a significant and inverse relationship between serum GH and hypertension, meaning LOWER levels of GH were actually associated with HIGHER levels of blood pressure (hypertension).
To be clear, I dont think in any way MK-677 is some cardio healthy or protective treatment, actually I doubt its healthy for your cardiovascular system at all but when it pertains to blood pressure, based on the science MK administration likely wouldn’t raise blood pressure.
EFFECT ON CANCER CELLS
Cancer cells are cells that divide continuously, eventually forming tumors. This is a result of abnormalities in the mechanisms that regulate normal cell proliferation. IGF-1 has been clearly shown to have proliferative effects. It binds to its IGF-1R receptor on cells and activates signaling pathways (PI3K/AKT and MAPK pathways) that drive cells to grow and divide. So by taking MK-677 and increasing IGF-1 levels you may cause existing cancer cells to grow and divide faster.
Essentially if, and only if you have existing cancer cells MK-677 could theoretically perpetuate the spread of cancer and lead to death. For this reason, Metformin is used to treat cancer (it reduces the levels of IGF-1 in the bloodstream).
Skin cancers respond particularly to IGF-1 and its growth pathways.
Interestingly there is actually evidence in the contrary with a study titled ‘Agonists of growth hormone-releasing hormone (GHRH) inhibit human experimental cancers in vivo by down-regulating receptors for GHRH’ where a GHRH agonist actually inhibited a certain type of cancer, however GHRH differ in their mechanism of action so its unclear whether these benefits can be attributed to MK-677. The level of concern should depend on age, race, genetic predisposition, smoking habits, and sun exposure.
EFFECT ON GYNECOMASTIA
Just to be clear I don’t think MK-677 will lead to the formation of Gyno, the only reason I want to discuss this topic is partly to address anecdotes claiming MK-677 caused Gyno, and also partly because of some interesting research on this topic. It was speculated it had something to do with Prolactin but studies have shown MK-677 to have a negligible effect on Prolactin levels.
Previously it had been shown that an infusion of IGF-1 into the brains of rodents caused an upregulation of Estrogen Receptor Alpha (NR3A1) in the hippocampal cells of the rodents brain. Upon realizing this, it was understood that in rodent brains the estrogen receptors were frequently co-located with IGF-1 receptors within the same cell. This is why when IGF-1 increases in the brain the Estrogen receptor could be activated, and Estrogen Receptor expression could increase in the presence of IGF-1.

This draws a very vague line between IGF-1 and gyno formation, as the formation of gyno is from the triggering of estrogen receptors in male breast tissue, and if IGF-1 and estrogen receptors are co-located in the hippocampal cells then they could be co-located in these cells too but there is no evidence as of yet and this is just speculation on how it could potentially happen. Overall I don’t believe MK-677 would form gyno because there isn’t any evidence that these receptors are co-located in male breast tissue but it is an interesting line of inquiry nonetheless.
EFFECTS ON LETHARGY AND BRAIN FOG
Lethargy is another common side effect reported anecdotally but not in any studies on MK-677, and yet again shows there is a place for considering anecdotes within science despite ranking lowest on the scientific hierarchy of evidence.
Anecdotes provide valuable lines of inquiry and insight, and may help shape future studies. In clinical trials, researchers may not realize a side effect of a compound simply because they weren’t looking for (measuring) it, and in this instance it was lethargy.

Anyways, the way lethargy is triggered by MK-667 administration hasn’t really been explained online. My opinion on why this occurs is as follows. As explained previously, MK-677 works by binding to the GHS-R1A receptor (a growth hormone secretagogue receptor), by mimicking Ghrelin. What is interesting is that this GHS-R1A receptor interacts with other receptors in the body, and has shown to join with other receptors such as receptors for things like dopamine, serotonin, oxytocin, orexin, or somatostatin.
When these receptors pair up they form something called ‘heterodimers’, and they influence each other’s signaling pathways.
For instance, Serotonin receptors can reduce the activation of GHSR when ghrelin tries to trigger it.

On the flip side, GHSR can change how dopamine receptors send signals, depending on the substance that binds to them. GHSR also interacts with a protein called MRAP-2, which improves the receptor’s response when ghrelin is present but lowers the receptor’s background activity when ghrelin isn’t around. As you can see the body has an extremely complex system to how it responds to hormones and response-regulation.
My proposition on how this works revolves around the serotonin receptors.
Serotonin has recently been shown to play a much bigger part in motivation pathways than originally thought, and helps regulate mood and wakefulness. The GHS-R1A receptor has been shown to interact with the 5-HT2c receptor (a serotonin receptor).

When MK-677 activates GHSR, it may interact with how the serotonin receptor works. If MK-677 over-activates GHSR (which is entirely possible as at the end of the day this is not a natural compound your body produces), this could interfere with serotonin’s usual function, possibly tipping the balance toward causing lethargy instead of wakefulness.
One common method of reducing the lethargy experienced by Mk-677 is by taking it right before bed, instead of in the morning. This administration ensures you experience the full benefits of its sleep improvement qualities, and its been proposed that by taking at night, before bed, you essentially ‘skip’ the wave of the lethargy people typically experience after administration. There’s no scientific explanation to prove whether this works or not but ultimately I’ve seen enough people claim by doing this they effectively eliminated the lethargy side effect, so its definitely something you should consider if your thinking of taking MK-677 and ultimately its up to your individual experience and discretion.
EPIGENETIC CHANGES
The winter of 1944-45, known as the “Hunger Winter” in the Netherlands, followed years of Nazi German occupation, which began in 1940. To support the Allies, the Dutch government-in-exile in London urged a national railway strike to disrupt German military efforts. In response, German authorities cut off food supplies to the occupied western region in October 1944.
The Dutch population was usually well-nourished before and after the Hunger Winter, which provided the conditions for the famine to be sort of a “natural experiment.”, allowing researchers to study the effect of this acute yet extreme famine on the subsequent generation. The conditions seen in this part of history essentially allowed researchers to study how environmental conditions you simply couldn’t replicate ethically in modern times had an effect on epigenetics.

In simple terms; these unique events in history allowed researchers to study how a mother’s undernutrition during specific stages of pregnancy might impact the health and life outcomes of children who were in the womb during this period.
The study that looked at this event is called ‘Cohort Profile: The Dutch Hunger Winter Families Study’.
One of the results that seemed antithetical at first was the prevalence of obesity in the subsequent generation, but it makes sense when you think about Ghrelin, and also the general nature of epigenetics.
For the large majority of it, people had to ration and spread 500kcal out each day.
One could reason that the levels of hunger could be described as both unbearable and prolonged or essentially ‘chronically extremely high’, and thus experienced persistently elevated Ghrelin levels. As a result, through the various processes involved in epigenetics (triggered gene methylation at ghrelin receptor genes), the children who experienced the famine ‘in-utero’ would have had inherited these chronically high ghrelin levels. As you can imagine, having these chronically high ghrelin levels, paired with the immediate availability of food after the year long war influenced famine, very simply explains this doubling in the rate of obesity (this was only studied in men but very likely extended to women too).

An interesting proposition I’d like to share is that potentially by artificially inflating your amount of Ghrelin receptor antagonism via MK-677 you may cause epigenetic changes that lead to obesity in your offspring. To be honest I think it is unlikely, but it is a theory you should be aware of.
MISCELLANEOUS
What is the recommended dose of MK-677?
In Human trials it’s been dosed between 10-50mg, but typically it was taken at 25mg and most sellers on the gray market sell it at 25mg. It is a common practice to start with 12.5mg a day by splitting the pills in half using a pill cutter, in order to reduce the extreme water retention that occurs most within the 1st week.
What is the half life of MK-677?
6 hours.
Is MK-677 a SARM?
No, it is commonly associated with SARMS but it is not. It has a few different classifications such as growth hormone secretagogue but it can be best defined as a Ghrelin Mimetic or Ghrelin receptor agonist.
What are some compounds similar to MK-677?
Ghrelin receptor agonists similar to MK-677 include
- GHRP-2 – has a significant effect on cortisol and prolactin levels and is administered via injection
- GHRP-6 – elicits a more significant appetite inducing effect than MK-677
- Ipamorelin – Ipamorelin is highly selective and is known to only elicit a GH response but it is administered by Injection. Has a low side effect profile.
- Anamorelin
- Hexarelin
- Capromorelin (usage available for cats and dogs to increase appetite and IGF-1). Human trials were discontinued in 2017.
- Adenosine (does not trigger Gh secretion but does initiate a hunger response)
- Macimorelin (AEZS-130, JMV 1843): Used in diagnostics to test for growth hormone deficiency
A very common protocol is combining Ipamorelin with something called CJC-1295.
CJC-1295 and Ipamorelin have slightly different mechanisms of actions which combine together to create a synergistic (1+1=3) effect.
CJC-1295 works by binding to the very confusing sounding growth-hormone-releasing-hormone receptor, and Ipamorelin works by binding to the GHSR-1A receptor. So they both bind to different receptors which both work to secrete GH. They also have different responses in GH secretion. CJC-1295 seems to increase baseline amounts of GH, while Ipamorelin enhances the amount of GH released in the GH pulses.
What are some typical protocols including MK-677?
Some common protocols employed with MK-677 are as follows;
- MK-677 combined with LGD-4033. Seen earlier in this article with a study evaluating the effect of their dual action
- MK-677 is commonly combined with SLIN pills or insulin mimetics. Full disclosure I haven’t studied SLIN pills in depth, but essentially they are taken with MK-677 because they supposedly provide a synergistic (1+1=3 effect), however personally I don’t think this popular protocol makes logical sense. Because of Mk’s appetite stimulating effect it is used during a bulk phase, but Slin pills hinder muscle growth because they promote AMPK and inhibit MTOR.
- Diuretics are commonly taken with MK-677 to reduce water retention – some natural diuretics taken are dandelion root, black & green tea, asparagus, and caffeine.
- Appetite suppressants are typically taken with MK-677 for someone trying to cut whilst using MK-677 for its muscle-sparing properties
- Some people in bodybuilding circles have theorized Huperzine A (200mcg x3/day) might boost the effects of MK-677. Some research papers show that Huperzine A could block somatostatin in the body. Similar to how myostatin will inhibit muscle growth, Somatostatin acts as a counterbalance to keep HGH levels from rising too high.
Do GH/IGF-1 levels return to baseline after use?
Yes
How does administration timing affect your experience with MK-677?
Something obscure about MK-677 is that it lasts around 24 hours, so most people just take it once a day. But since it releases GH and IGF-1 in pulses throughout the day, it ends up acting more like the body’s natural GH cycle, making the timing of each dose less important than with other GHS compounds.
Also many anecdotes report that administration before bed helps reduce lethargy experienced by MK-677, whilst enhancing sleep quality.
Can MK-677 increase height?
Yes it can increase height but only if you’re still going through puberty and have not reached height maturation.
What is the biggest risk factor when taking MK-677?
It depends on the duration of exposure. For shorter cycles the biggest risk is its impact on blood sugar, so I would recommend taking regular blood glucose tests. Its extreme water retention can also be risky in the shorter term. In the longer term (1+ years) I would worry about its effects on the cardiovascular system.
Does MK-677 affect cortisol?
Unlike most GH secretagogues, MK-677 does not elevate cortisol.
Is research on MK-677 ongoing?
Yes, research on MK-677 is still ongoing, but under the new name LUM-201. The name changed as after the right to a compound was transferred between pharmaceutical companies they also changed its name to identify it within their large catalog of research compounds.
LUM-201 is being researched by company ‘Lumos Pharma’ for treating ‘Prepubertal Children With Idiopathic Growth Hormone Deficiency’.
What is the history of MK-677?
GHRPs (growth hormone releasing peptides) were first synthesized in 1977. They were discovered when scientists were researching natural opioids (endorphins) which agonize the opioid receptors in the brain, and they began creating synthetic versions of them and eventually noticed one that caused growth hormone to be released in rodents, GHRP6.
GHRP6 was the first that was shown to have clinical usage as it had significant in vivo activity. However due to having very low oral bioavailability, and also its short half-life as mentioned previously, it could only be administered via frequent injection which are as you can imagine very undesirable.
Because of its shortcomings, Merck Pharmaceuticals stopped its development instead opting to use its model structure as a sort of blueprint to develop a non-peptide mimetic that could be administered orally (high bioavailability) and with a longer half-life (allowing for once daily oral administration).
Eventually they synthesized a compound called L-692,429 which acted as a peptidomimetic agonist of GHRP6. Continued modifications then led to L-163,191, and then eventually the development of L-163,191 (or MK-677). MK-677 was shown to elevate levels of IGF-1 for 24 hours which Merck was looking for.
Merck discontinued development in 1999, and it was then acquired by Ammonett Pharma, then in 2018 it was acquired by Lumos Pharma who is continuing to study it.
On an unrelated note, when GHRPs and GHS were discovered, Ghrelin and its role in GH release hadn’t been discovered yet, so MK-677 was first categorized as a growth hormone secretagogue as a result, however the better classification of MK-677 is as a ghrelin mimetic.
Where can I buy MK-677?
MK-677 is one of the most commonly bought compounds of the gray market. It is available online, but this has its own risks and may be illegal depending on what country you’re living in. Dodgy SARM companies will often claim their compounds, including MK-677, are third party tested and provide these tests for your batch bought, however these are easily faked and there is no guarantee you are getting what you pay for. I would recommend to stay away from these companies, however if you are determined to get some MK-677, do your own research and use your own discretion in determining which companies are the most reliable even if you have to pay slightly more.
Will MK-677 lower my testosterone levels?
No it won’t.
How long will MK-677 affect my appetite after cessation?
In patients that took MK-677 for a year it was reported for half the patients the increased appetite persisted for 3 months after cessation, and longer in others. It would be safe to assume that the appetite persistence would last 1/4 of whatever the length of exposure to MK-677 was, but potentially in shorter cycles it would return to baseline faster.
What are the effects on combining MK-677 with a myostatin inhibitor?
Combining MK-677 with a myostatin inhibitor (for example YK-11) could theoretically boost muscle growth more than each on its own due to a theoretical synergistic (1+1=3) effect. However we don’t have much research on how these work together in humans, so we don’t fully understand the long-term safety.
What are some advantages of taking MK-677 rather than growth hormone?
Firstly, the method of administration. MK-677 can just be taken once daily in an oral tablet which is easy to do and much more desirable than injection of growth hormone.
MK-677 is also much cheaper than pharma grade growth hormone.
Another difference most people overlook is the speed at which the increase in BMR becomes apparent. As mentioned there was a 1998 study on obese patients that found that MK-677 administration led to a significant increase in BMR after just two weeks, which is much faster than traditional GH administration which was shown to take two months in a study on pre-pubertal boys.
Should MK-677 be taken in a bulking phase, cutting phase, or maintenance phase?
Users should take it with their own discretion however most anecdotes take it during a bulking phase.
Sources:
https://pmc.ncbi.nlm.nih.gov/articles/PMC2757071/
https://pubmed.ncbi.nlm.nih.gov/11715022/
https://pubmed.ncbi.nlm.nih.gov/28533420/
https://pmc.ncbi.nlm.nih.gov/articles/PMC7564605/#B25-cells-09-01970
https://pubmed.ncbi.nlm.nih.gov/7990709/
https://pmc.ncbi.nlm.nih.gov/articles/PMC6373369/#CR30
https://pubmed.ncbi.nlm.nih.gov/9467542/
https://pmc.ncbi.nlm.nih.gov/articles/PMC8706217/
https://pubmed.ncbi.nlm.nih.gov/29765966/
https://ib.bioninja.com.au/adaptive-immunity/
https://pmc.ncbi.nlm.nih.gov/articles/PMC8666548/
https://pubmed.ncbi.nlm.nih.gov/10592455/
